
Page 21 - RUFARS 2021 - Proceedings
P. 21
ISSN: 2659-2029
Proceedings of the 4 Research Symposium of the Faculty of Allied Health Sciences
th
University of Ruhuna, Galle, Sri Lanka
August 26, 2021
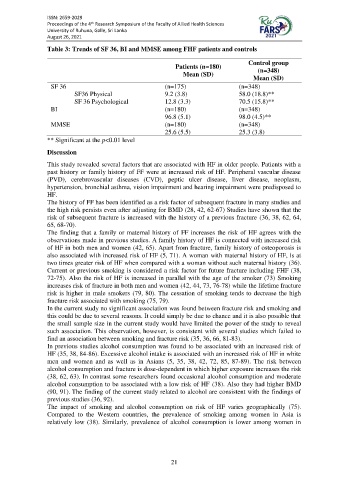
Table 3: Trends of SF 36, BI and MMSE among FHF patients and controls
Control group
Patients (n=180) (n=348)
Mean (SD)
Mean (SD)
SF 36 (n=175) (n=348)
SF36 Physical 9.2 (3.8) 58.0 (18.8)**
SF 36 Psychological 12.8 (3.3) 70.5 (15.8)**
BI (n=180) (n=348)
96.8 (5.1) 98.0 (4.5)**
MMSE (n=180) (n=348)
25.6 (5.5) 25.3 (3.8)
** Significant at the p<0.01 level
Discussion
This study revealed several factors that are associated with HF in older people. Patients with a
past history or family history of FF were at increased risk of HF. Peripheral vascular disease
(PVD), cerebrovascular diseases (CVD), peptic ulcer disease, liver disease, neoplasm,
hypertension, bronchial asthma, vision impairment and hearing impairment were predisposed to
HF.
The history of FF has been identified as a risk factor of subsequent fracture in many studies and
the high risk persists even after adjusting for BMD (28, 42, 62-67) Studies have shown that the
risk of subsequent fracture is increased with the history of a previous fracture (36, 38, 62, 64,
65, 68-70).
The finding that a family or maternal history of FF increases the risk of HF agrees with the
observations made in previous studies. A family history of HF is connected with increased risk
of HF in both men and women (42, 65). Apart from fracture, family history of osteoporosis is
also associated with increased risk of HF (5, 71). A woman with maternal history of HF, is at
two times greater risk of HF when compared with a woman without such maternal history (36).
Current or previous smoking is considered a risk factor for future fracture including FHF (38,
72-75). Also the risk of HF is increased in parallel with the age of the smoker (73) Smoking
increases risk of fracture in both men and women (42, 44, 73, 76-78) while the lifetime fracture
risk is higher in male smokers (79, 80). The cessation of smoking tends to decrease the high
fracture risk associated with smoking (75, 79).
In the current study no significant association was found between fracture risk and smoking and
this could be due to several reasons. It could simply be due to chance and it is also possible that
the small sample size in the current study would have limited the power of the study to reveal
such association. This observation, however, is consistent with several studies which failed to
find an association between smoking and fracture risk (35, 36, 66, 81-83).
In previous studies alcohol consumption was found to be associated with an increased risk of
HF (35, 38, 84-86). Excessive alcohol intake is associated with an increased risk of HF in white
men and women and as well as in Asians (5, 35, 38, 42, 72, 85, 87-89). The risk between
alcohol consumption and fracture is dose-dependent in which higher exposure increases the risk
(38, 62, 63). In contrast some researchers found occasional alcohol consumption and moderate
alcohol consumption to be associated with a low risk of HF (38). Also they had higher BMD
(90, 91). The finding of the current study related to alcohol are consistent with the findings of
previous studies (36, 92).
The impact of smoking and alcohol consumption on risk of HF varies geographically (75).
Compared to the Western countries, the prevalence of smoking among women in Asia is
relatively low (38). Similarly, prevalence of alcohol consumption is lower among women in
21